Editor’s Note: Lost&Found is beginning a regular series of articles and podcasts about research and best practices in mental health, resilience, and suicide prevention. This first article is an overview of the idea of suicide prevention as something that requires a public health approach, as well as of the seven prevention strategies that our work is based on.
Read and download this article as a printable PDF by clicking on the image above.
“Suicide is a public health problem,” U.S. Surgeon General Satcher wrote in 1999, adding that suicide prevention requires a public health approach.
While suicide is—by definition—an individual act, suicide affects and is influenced by all levels of society—individuals, their relationships, communities, and society as a whole. This understanding of suicide as part of a larger system is the basis for the suicide prevention strategies developed by the Centers for Disease Control and Prevention, and those strategies in turn are the basis for the programs developed and implemented by Lost&Found.
This article gives a brief history of this approach to suicide prevention and an overview of the CDC’s seven suicide prevention strategies. Future articles will look more closely at the seven strategies and the Lost&Found programs that are working to carry them out.
Suicide prevention as a societal concern: A brief history
Who can prevent a suicide?
If you had asked this question in 1958, when the first suicide prevention center in the United States opened in Los Angeles (Morris, 2011), the answers probably would have been limited to a small circle of people: The people with suicidal ideation themselves; perhaps the people closest to them, who may have noticed signs or who were confided in; and those who were trained in crisis intervention.
The rest of society could sympathize and support, perhaps, but for most people, there was no active role to play unless (and one hoped it never happened) thoughts of suicide struck them or a loved one.
By the late 1990s, that view was changing. A key pivot point was in 1998, when stakeholders gathered in Reno, Nevada, for the first National Suicide Prevention Conference (U.S. Public Health Service, 2001), which resulted in 81 recommendations for action. The key points from the conference indicated a shift in suicide prevention from solely focusing on individuals to recognizing the role that society more broadly could play in preventing suicide:
- Suicide prevention must recognize and affirm the value, dignity, and importance of each person.
- Suicide is not solely the result of illness or inner conditions. The feelings of hopelessness that contribute to suicide can stem from societal conditions and attitudes. Therefore, everyone concerned with suicide prevention shares a responsibility to help change attitudes and eliminate the conditions of oppression, racism, homophobia, discrimination, and prejudice.
- Some groups are disproportionately affected by these societal conditions, and some are at greater risk for suicide.
- Individuals, communities, organizations, and leaders at all levels should collaborate to promote suicide prevention.
- The success of this strategy ultimately rests with individuals and communities across the United States. (Office of the Surgeon General, 2012)
In 1999, then-U.S. Surgeon General Dr. David Satcher issued a national call to action developed from the findings from the Reno conference. It included this explanation of a view of suicide prevention that looks beyond the individual:
“Suicide is a public health problem that requires an evidence-based approach to prevention. In concert with the clinical medical approach, which explores the history and health conditions that could lead to suicide in a single individual, the public health approach focuses on identifying and understanding patterns of suicide and suicidal behavior throughout a group or population. The public health approach defines the problem, identifies risk factors and causes of the problem, develops interventions evaluated for effectiveness, and implements such interventions widely in a variety of communities.” (U.S. Public Health Service, 1999)
In 2000, a Federal Steering Group was formed to respond to this call to action, which resulted in the publication of the National Strategy for Suicide Prevention in 2001. It included 11 goals and 68 objectives based on the framework Satcher had put forward in the call to action. The strategy document was a planted flag of sorts for those working in suicide prevention, giving them a common understanding and language to work from, as well as a way to direct attention and resources to suicide prevention efforts. One result of this strategy, for example, was the development of the National Suicide Prevention Lifeline (800-273-TALK/8255), which connects callers to a responder at the closest crisis center.
Gathering evidence and best practices
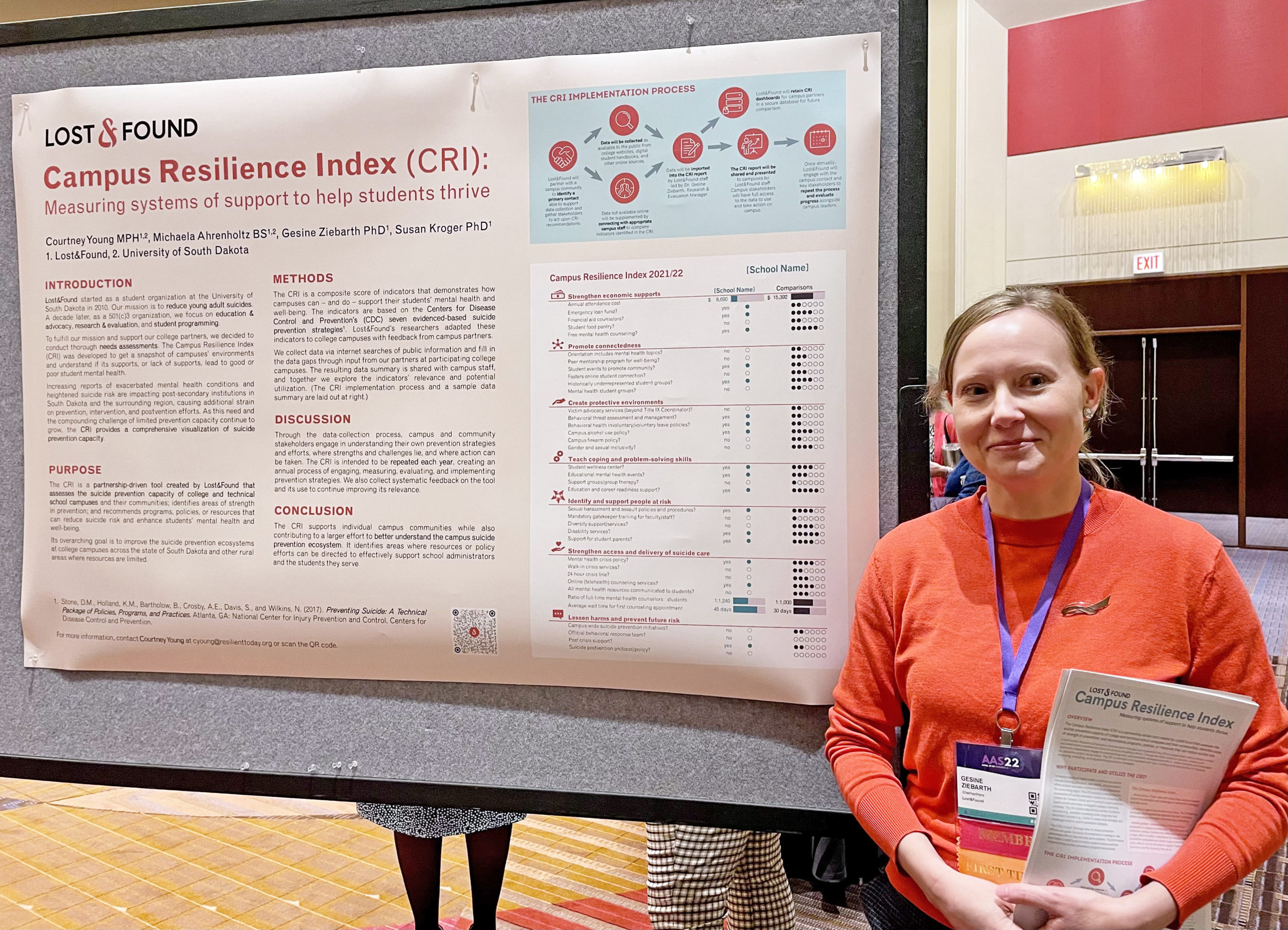
Over the past 21 years, the public health understanding of suicide prevention has increasingly shaped the progress and development of the field, and researchers have gathered evidence of what public health approaches are effective. In 2017, the CDC published Preventing Suicide: A Technical Package of Policy, Programs, and Practices (Stone et al, 2017). Like other technical packages produced by the CDC, the document compiles a set of strategies that communities can use to achieve a desired outcome—in this case, the prevention of suicide—along with specific approaches to advance the strategy, as well as evidence for why those strategies work. This technical package guides much of the suicide prevention work happening now across the United States, including the programs offered by Lost&Found.
Dr. Deb Stone of the Division of Violence Prevention at the Centers for Disease Control and Prevention is one of the authors of the technical package and spoke with Lost&Found in a phone interview (Stone D., 2022).
The process of creating the technical package involved a review of the literature and many conversations with subject matter experts, Stone explained. “We really looked for programs, practices, and policies that showed evidence for reducing actual suicide or suicide attempts, or that impacted on suicide risk and protective factors. The evidence we found … had to come from rigorous scientific studies such as meta-analyses or systematic reviews, or from randomized, controlled trials, just to name a few of the types of studies that we were looking at.”
The public health approach underlying this work meant that the researchers had a broad view of whom to target with their efforts. This includes people all along the timeline of a suicide.
“We knew that we needed to find strategies that would help to prevent suicide risk in the first place—sometimes called primary prevention or upstream prevention,” Stone said. “We wanted to help support people who were already at increased risk, and then also work to prevent re-attempts among people who may have attempted, and help support people who have suffered a suicide loss.”
Another viewpoint that is critical to the understanding of suicide prevention, Stone said, is recognizing that, while suicide is an individual act and is influenced by factors in that individual, it is also influenced by factors in a person’s relationships, the community, and society at large.
“The contributors or the causes of suicide occur at the individual, relationship, community, and societal levels, and those four levels comprise the social ecological model,” Stone said.
For example, at the individual level, people with mental health challenges, substance use, or who have attempted suicide in the past are at increased risk of suicide. At the relationship level, a recent breakup, the death of a loved one, or having been the victim of violence increase risk. At the community level, increased risk can result from difficulty accessing mental health care. And at the societal level, suicide risk is affected by whether policies allow easy access to lethal means such as firearms and medications, as well as societal stigmas around mental illness or seeking help.
“To have the biggest impact, we may need to consider strategies that will address factors across all these levels,” Stone said. “Sometimes, that’s where we get stuck, because we might only focus on one thing, but we really need to be taking a broader perspective and a broader approach.”
This wider view can help to combat a common misconception about suicide—that it is based on a single factor.
“In our desire to understand why someone would take their own life, we sometimes rush to conclusions and point to one thing,” Stone said. “But this really minimizes what the person was going through, and data tell us … that there are many factors involved. And so, if we’re going to prevent suicide, we really need to consider all of these factors.”
Another common misconception about suicide is that a person who dies by suicide was weak or selfish, and an evidence-based public health approach suggests ways to combat this misconception as well.
“People who are struggling with thoughts of suicide are in immense emotional and sometimes physical pain. And this pain is typically related to the culmination or a confluence of many factors. So when you’re in this level of pain, the options and the solutions can become so narrowed that suicide may seem to be the only way out,” Stone said. “We want to prevent people from ever getting to the point of having a crisis like that. We want to prevent situations that spurred these crises from occurring in the first place.
“But if we are past that point, there’s still a lot we can do to help people. We can help destigmatize getting help … and we can make sure that professionals are equipped with ways of helping people in suicidal crisis by training on effective approaches for suicide prevention. And then we can all, working together in a society, learn the warning signs and ask the hard questions. ‘Are you thinking about suicide?’ We know that this will not put the thought in someone’s head, and it can actually break the silence that is so detrimental.”
The CDC’s seven strategies for suicide prevention
The CDC’s technical package on suicide prevention distills its recommendations into seven strategies that “are intended to work in combination and reinforce each other to prevent suicide,” according to the document (Stone et al, 2017, p. 12). The strategies, as a whole, approach suicide prevention at all four levels of the social ecological model (individual, relationships, communities, and society).
What follows is a summary of each of these strategies from the CDC document and one or two key approaches to implementing that strategy.
Strategy 1: Strengthen economic supports.
Economic and financial strain, such as job loss, long periods of unemployment, reduced income, difficulty covering medical, food, and housing expenses, and even the anticipation of such financial stress may increase an individual’s risk for suicide or may indirectly increase risk by exacerbating related physical and mental health problems. Buffering these risks can, therefore, potentially protect against suicide. (Stone et al, 2017, p. 15)
“We sometimes forget the real devastation that can impact people and that people can feel due to financial and economic concerns,” Stone said.
Some of the ways to improve those situations and help prevent suicide include increases to the minimum wage and policies that allow people to stay in their homes or find secure housing.
Strategy 2: Strengthen access and delivery of suicide care.
[M]ental illness is an important risk factor for suicide. State-level suicide rates have also been found to be correlated with general mental health measures such as depression. Findings from the National Comorbidity Survey indicate that relatively few people in the U.S. with mental health disorders receive treatment for those conditions. (Stone et al, 2017, p. 19)
“This strategy is focused on making sure that all people have access to quality care, especially in underserved areas such a rural communities, and that once people are engaged in care, that they don’t fall through the proverbial cracks as they transition in and out of the healthcare system,” Stone said.
One approach for implementing this strategy is remote mental health care, also called telemental health, which became more common during the Covid-19 pandemic. Another is ensuring that mental health conditions are covered in health insurance policies.
Strategy 3: Create protective environments.
Prevention efforts that focus not only on individual behavior change (e.g., help-seeking, treatment interventions) but on changes to the environment can increase the likelihood of positive behavioral and health outcomes. Creating environments that address risk and protective factors where individuals live, work, and play can help prevent suicide. (Stone et al, 2017, p. 23)
One way in which the environment can be addressed in terms of suicide prevention is access to lethal means.
“We know that reducing access to lethal means such as a firearms, especially among people at risk of suicide, can really make all of the difference in saving someone’s life,” Stone said, because “putting time and space between someone who is thinking about suicide and the means to carry it out is absolutely critical.”
Another approach is improving policies and social norms around help seeking—both allowing and encouraging people to take time off from work to seek mental health care, for example.
Strategy 4: Promote connectedness.
[S]tudies suggest a positive association between social capital (as measured by social trust and community/neighborhood engagement), and improved mental health. Connectedness and social capital together may protect against suicidal behaviors by decreasing isolation, encouraging adaptive coping behaviors, and by increasing belongingness, personal value, and worth, to help build resilience in the face of adversity. Connectedness can also provide individuals with better access to formal supports and resources. (Stone et al, 2017, p. 27)
“As far back as the late 1880s, we had this great sociologist, Emile Durkheim, who told us that social connectedness … is a protective factor. And what that means is that it can protect people from ever becoming suicidal in the first place, and it can reduce the chances that someone would ever attempt suicide,” Stone said.
Stone would like to see more research in this area, since the limited research on connectedness and mental health is promising. For example, people working together on a community greening initiative showed reductions in anxiety and depression. “In addition, pride in the community would increase, and people would support each other through those kinds of engagement activities,” she said.
The Covid-19 pandemic limited our usual ways of connecting, which shows what can happen when the connectedness we typically rely on isn’t available: Anxiety and depression increased 25 percent worldwide in the first year of the pandemic, according to a brief by the World Health Organization (Brunier, 2022). The stress of social isolation was cited as one of the causes.
Strategy 5: Teach coping and problem-solving skills.
The inability to employ adequate strategies to cope with immediate stressors or identify and find solutions for problems has been characterized among suicide attempters. Teaching and providing youth with the skills to tackle everyday challenges and stressors is, therefore, an important developmental component to suicide prevention. (Stone et al, 2017, p. 31)
“We know that teaching people—not just kids, but kids and adults—how to cope and solve conflicts can really go a long way to preventing crises that sometimes escalate to the point that someone is thinking about suicide,” Stone said. “It’s not often discussed, but problems in relationships such as bullying or breakups or other kinds of conflicts are some of the most common contributors to suicide. And many of us were, frankly, never really taught how to cope with conflict or how to problem-solve. But the good news is that there are skills that we can all learn and excel at with practice.”
Programs that teach these life skills to children are having payoffs down the road in preventing the risk of suicide and other adverse outcomes. These programs could be scaled up and expanded to reach more people, including adults, Stone said.
Strategy 6: Identify and support people at risk.
In order to decrease suicide, care of, and attention to, vulnerable populations is necessary, as these groups tend to experience suicidal behavior at higher than average rates. Such vulnerable populations include, but are not limited to, individuals with lower socio-economic status or who are living with a mental health problem; people who have previously attempted suicide; veterans and active duty military personnel; individuals who are institutionalized, have been victims of violence, or are homeless; individuals of sexual minority status; and members of certain racial and ethnic minority groups. (Stone et al, 2017, p. 35)
This strategy works to support people who are at high risk of suicide or who are known to have thoughts of suicide. The good news is that treatments are showing great promise in helping with mental health conditions and reducing the suicide risk.
“The evidence for different forms of therapy, such as cognitive behavior therapy, especially with collaborative care components, is really mounting, and that’s really exciting,” Stone said.
An approach to implement this strategy is to continue the research for these programs and to provide more training for practitioners.
Strategy 7: Lessen harms and prevent future risk.
Millions of people are bereaved by suicide every year in the United States and throughout the world. Risk of suicide and suicide risk factors has been shown to increase among people who have lost a friend/peer, family member, co-worker, or other close contact to suicide. Care and attention to the bereaved is therefore of high importance. Despite often good intentions, media and others responding to suicide may add to this risk. (Stone et al, 2017, p. 41)
This strategy aims to help people after a suicide has taken place. This includes people who were directly connected to the person who died by suicide, ensuring that they receive support and can access professional mental health care if they need it. This strategy also includes those in the community or society more broadly who hear that a suicide has happened. One important way to implement this strategy is to learn better ways to talk about suicide, especially for those in the media.
“We still have a long way to go in safe reporting,” Stone said. “This really means avoiding sensationalizing a suicide, describing the details or means of suicide, or glamorizing somebody who died by suicide, because we know that those things can inadvertently increase risk for people who may be vulnerable or thinking about suicide themselves. … This is an area where we can continue to promote positive messaging and resources and make sure to get people the help that they need.”
Looking ahead
A lot has happened in the world and in the field of suicide prevention in the nearly five years since the CDC’s technical package of suicide prevention strategies was released. While not all the developments have been positive, many significant findings and events of the past five years have strengthened the evidence for and emphasized the importance of a public health approach to suicide prevention.
Perhaps the biggest change has come from the Covid-19 pandemic, which changed the way that people live, work, and gather with friends and family. Many have died from the virus, so many others are dealing with grief; many are dealing with poorer health because of long Covid; and many immunocompromised people remain socially isolated because the risk of Covid remains high for them. These changes have affected mental health across the globe (World Health Organization, 2022). “There are increases in anxiety and substance use and distress, and even in suicidal thinking, particularly among young people but also among people who have been disproportionately impacted by Covid-19,” Stone said.
The CDC is working on a new release of the technical package, to be made public sometime this year. The seven strategies will remain, Stone said, backed up by new evidence. Some of this is based on improvements in data collection—researchers now have the ability to track and monitor data related to suicide ideation and suicide attempts in closer to real time, Stone said, and machine learning can help to forecast suicide trends in the future. New studies have also provided additional evidence to support some of the programs and policies recommended in the 2017 report, as well as evidence to support new programs and policies.
Stone is also looking forward to the way that the development and promotion of a three-digit number (988) for the National Suicide Prevention Lifeline will increase support for people with suicidal thoughts. That number will go live in July.
“We have a long way to go, but we’re certainly making great strides to help individuals and communities reduce this incredible burden of suicide,” Stone said.
References
Brunier, A. D. (2022, March 2). Covid-19 pandemic triggers 25% increase in prevalance of anxiety and depression worldwide. Retrieved from World Health Organization website: https://www.who.int/news/item/02-03-2022-covid-19-pandemic-triggers-25-increase-in-prevalence-of-anxiety-and-depression-worldwide
Morris, L. (2011). History of the Suicide Prevention Center. Los Angeles Suicide Prevention Summit, (pp. 5-6). Los Angeles, CA. Retrieved from http://file.lacounty.gov/SDSInter/dmh/166651_HistoryoftheSuicidePreventionCenter.pdf
Office of the Surgeon General. (2012). Appendix C: Brief History of Suicide Prevention in the United States. 2020 National Strategy for Suicide Prevention: Goals and Objectives for Action. Washington, DC: Office of the Surgeon General (US); National Action Alliance for Suicide Prevention (US). Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK109918/
Stone, D. (2022, January 27). Interview with Dr. Deb Stone. (H. Marttila-Losure, Interviewer)
Stone, D.M., Holland, K.M., Bartholow, B., Crosby, A.E., Davis, S., and Wilkins, N. (2017). Preventing Suicide: A Technical Package of Policies, Programs, and Practices. Atlanta, GA: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention. Retrieved from https://www.cdc.gov/violenceprevention/pdf/suicideTechnicalPackage.pdf
U.S. Public Health Service. (1999). The Surgeon General’s Call to Action to Prevent Suicide. Washington, DC. Retrieved from https://sprc.org/sites/default/files/migrate/library/surgeoncall.pdf
U.S. Public Health Service. (2001). National Strategy for Suicide Prevention: Goals and Objectives for Action. Rockville, MD: U.S. Department of Health and Human Services. Retrieved from https://redmondschools.org/wp-content/uploads/2021/08/National_Strategy_for_Suicide_P.pdf
World Health Organization. (2022). Mental Health and COVID-19: Early evidence of the pandemic’s impact. Scientific brief. Retrieved from World Health Organization website: https://www.who.int/publications/i/item/WHO-2019-nCoV-Sci_Brief-Mental_health-2022.1